I looked at the numbers to check whether this was a fair allocation of funds and how the CARES funds were allocated in the first place.
CARES $$
Population
Total COVID cases*
COVID cases/100K*
USA
150,000,000,000 (100%)
328,200,000 (100%)
1,030,487 (100%)
314
Suffolk
257,670,000 (1.72%)
1,477,000 (0.45%)
32,724 (3.2%)
2209
Nassau
236,790,000 (1.57%)
1,357,000 (0.41%)
35,085 (3.4%)
2584
* based on reports from end of April
First, although Suffolk and Nassau counties are flashpoints of the current COVID-19 outbreak with few other counties anywhere in the USA rivaling the numbers of cases per 100K population, neither county is getting the dollar amount reflecting that. Going by total COVID cases, they should be getting about 3.2-3.4% of the CARES dollars, but they are actually only getting about half of that.
So why is Lee Zeldin bragging about this? Is he perhaps suggesting that as the president’s friend and big supporter, he has procured a special deal for us? The numbers tell a different story: Long Island is getting squeezed.
Second, part of the problem is the method by which allocation was calculated:
This obviously skews the money allocation to the less populous states which are mainly red states.
“Local governments with populations of 500,000 or more (like Suffolk and Nassau) are also eligible for aid, a provision responsible for much of the confusion. Localities are permitted to claim 45 percent of the amount allocated for their population, while the state retains the other 55 percent as it also serves that population. The state also retains 100 percent of the amount allocated to populations not within a locality of 500,000 or more.” https://taxfoundation.org/federal-coronavirus-aid-to-states-under-cares-act/
The executive branch and the US Treasury Dep., in particular, are running this show. And allocations are determined by their formula. It is unclear to me how Lee Zeldin can claim any bragging rights for the money allocated to Suffolk county.
Should we not insist on having a congressional representative who actually fights for his constituents? Instead, we have a Trump imitator who all too often uses tragedy to promote himself and his political campaign.
What goes much further in my book is when credit is received from others and in particular from Democratic leaders. Here is an example from the East Hampton Star:
Mr. Steve Bellone, the Suffolk County Executive (a democrat) explained that The Municipal Liquidity Facility gives counties the ability to do short-term borrowing to address cash flow issues caused by revenue almost completely drying up because of the wholesale shutdown of certain parts of our economy. Previously, a county must have had at least two million residents, which Suffolk county does not, to qualify for the Municipal Liquidity Facility. So Bellone wrote a letter to Steve Mnuchin.
Mr. Bellone credited Senator Charles Schumer and Rep. Lee Zeldin with persuasive advocacy for Suffolk. Mr. Schumer “literally walked the letter into Steven Mnuchin’s office,” he said of his letter to the Treasury Secretary and spoke with Jerome Powell, the chairman of the Federal Reserve. Mr. Zeldin lobbied President Trump and Mr. Mnuchin, Mr. Bellone said, “and the congressman put me on the phone, set up a call with the Treasury secretary and himself so I could make the case directly about why Suffolk County needs this and why this is so important.”
By law, Lalota can’t run the BOE while running for office
Submitted by Jacquelyn Gavron
Following is testimony presented to the Legislature during its public hearing on an Independent Office of Inspector General for Suffolk County, proposed in response to pervasive corruption and conviction of Countyofficials and to the tragic death of 8-year old Thomas Valva, whose death raises questions of possible misconduct and mismanagement by County departments. (Statement Delivered to Suffolk County Legislature, April 28, 2020)
“Good afternoon. My name is Jacquelyn Gavron and I’m here to support the new Office of Inspector General, whose intent is to “identify and eradicate fraud, waste, abuse and corruption…to protect public integrity of government… and to safeguard the use of taxpayer dollars.” It is critical that election integrity be part of this effort. That’s why I’m informing you of a potential violation of NYS Election Law that requires your immediate attention.
“Nicholas Lalota, who was nominated and confirmed as Suffolk County Board of Elections Commissioner in January 2015 (and again in 2019), is running as Republican candidate for NYS Senate District 8 (Babylon Beacon). (Also see 2/20/20 announcement of candidacy.)
“On February 24, 2020 Commissioner Lalota announced he would take a leave of absence as of March 30, 2020. (Newsday, 2/23/20).
“However, under NYS Election Law section 3-200 (6), Commissioner Lalota was required to resign his office. That section provides:
6. An election commissioner shall not be a candidate for any elective office which he would not be entitled to hold under the provisions of this article, unless he has ceased by resignation or otherwise, to be commissioner prior to his nomination or designation therefor. Otherwise such nomination or designation shall be null and void.
“As the Board of Elections has ruled in Formal Opinion 1983, Opinion #4, 6/7/83 , a commissioner “must resign prior to the filing of his nominating or designating petitions.” A leave of absence does not satisfy the statute’s requirement that a commissioner has “ceased . . . to be commissioner . . .” While on a leave of absence, Commissioner Lalota still remains in office and retains control. In fact, he is still listed on the BOE website as the Republican Commissioner.
“In Lalota’s case, the apparent violation of sec. 3-200(6) is particularly disturbing because he is running for office in the same county over whose elections he has control.
“It would be egregious for any commissioner, Democrat or Republican, to stay in office in violation of the law, but it’s particularly outrageous for Lalota, around whom questions have swirled.
In 2018, Commissioner Lalota suspended walk-in absentee ballots, prompting County Executive Steve Bellone to write “a letter to the state Board of Elections. . .asking it to investigate the Suffolk BOE because the new policy was “disenfranchising voters.” (Newsday)
“And since 2017 Commissioner Lalota has been a part-time student at the [Maurice A. Deane] School of Law at Hofstra while earning a $144,000 salary for his full-time job as commissioner. According to Hofstra’s website, “. . . part-time classes . . . meet five days a week so that law school can be completed in four years.” Yet an 18-month audit by the Suffolk County Comptroller was unable to verify Commissioner Lalota’s time and attendance records.
The public is depending on your leadership [SC Legislature] and that of Suffolk County Executive Bellone, to ensure fair and safe elections, to protect public integrity of government, and to safeguard the use of taxpayer dollars.
“Thank you for your attention to this urgent matter.”
NOTE: Many thanks to Amy Turner for her invaluable assistance.
The Covid-19 pandemic is putting the deepening class divide in America into stark relief.
Four new classes are emerging.
The Remotes: These are professional, managerial, and technical workers – an estimated 35% of the workforce – who are putting in long hours at their laptops, Zooming into conferences, scanning electronic documents, and collecting about the same pay as before the crisis. Many are bored or anxious, but they’re well off compared to the three other classes.
The Essentials: They’re about 30% of workers, including nurses, homecare and childcare workers, farm workers, food processors, truck drivers, warehouse and transit workers, drugstore employees, sanitation workers, police officers, firefighters, and the military. Too many Essentials lack adequate protective gear, paid sick leave, health insurance, and childcare, which is especially important now that schools are shuttered. They also deserve hazard pay. Their vulnerability is generating a wave of worker activism at businesses such as Instacart, Amazon, Walmart, and Whole Foods. Mass-transit workers are organizing work stoppages. Trump’s Occupational Safety and Health Administration has the legal authority to require private employers provide essential workers with protective gear. Don’t hold your breath.
The Unpaid: They’re an even larger group than the unemployed – whose ranks could soon reach 25%, the same as in the Great Depression. Some of the unpaid are furloughed or have used up their paid leave. So far in this crisis, 43% of adults report they or someone in their household has lost jobs or pay, according to the Pew Research Center. An estimated 9.2 million have lost their employer-provided health insurance. Many of these jobs had been in personal services that can’t be done remotely, such as retail, restaurant, and hospitality work. But as consumers rein in spending, layoffs are spreading to news organizations, tech companies, and consumer-goods manufacturers. The unpaid most need cash to feed their families and pay the rent. Fewer than half say they have enough emergency funds to cover three months of expenses, according to a survey conducted this month by Pew. So far, government has failed them, too. Checks mailed out by the Treasury last week are a pittance. Extra benefits could help, but unemployment offices are so overwhelmed with claims that they can’t get money out the door. Loans to small businesses have gone largely to big, well-connected businesses, with banks collecting fat fees. On Wednesday, Republican Senate majority leader Mitch McConnell said he is opposed to any further federal aid to state and local governments, suggesting states declare bankruptcy instead. Which means even less money for unemployment insurance, Medicaid, and everything else the unpaid need. The resulting desperation is fueling demands to “reopen the economy” long before it’s safe. If it comes down to a choice between risking one’s health and putting food on the table, many will take the latter.
The Forgotten: This group includes everyone for whom social distancing is nearly impossible because they’re packed tightly into places most Americans don’t see: prisons, jails for undocumented immigrants, camps for migrant farmworkers, Native American reservations, homeless shelters, and nursing homes. While much of New York City is sheltering at home, for example, more than 17,000 men and women, many already in poor health, are sleeping in roughly 100 shelters for single adults. All such places are becoming hotspots for the virus. These people need safe spaces with proper medical care, adequate social distancing, testing for the virus and isolation of those who have contracted it. Few are getting any of this. Not surprisingly, the Essentials, the Unpaid, and the Forgotten are disproportionately poor, black, and Latino and they are disproportionately becoming infected. An Associated Press breakdown of available state and local data showed close to 33% of those who have died from Covid-19 are African American, despite representing only 14% of the total population in areas surveyed. The Navajo Nation already has lost more people to coronavirus than have 13 states. Four of the 10 largest-known sources of infection in the United States have been correctional facilities. These three groups aren’t getting what they need to survive this crisis because they don’t have lobbyists and political action committees to do their bidding in Washington or state capitals.
The Remotes among us should be concerned, and not just because of the unfairness of the Covid-19 class divide. If the Essentials aren’t sufficiently protected, the Unpaid are forced back to work earlier than is safe, and if the Forgotten remain forgotten, no one is secure. Covid-19 will continue to spread sickness and death for months, if not years to come.
This Tuesday, April 28 at 11 a.m. Pacific Time/2 p.m. Eastern Time, I’ll be having a live discussion with Stacey Abrams about the future of the Democratic Party and voting rights in the age of coronavirus. You can tune in here.
D. Posnett: Note for D. Trump and L. Zeldin: best to consider all of these 4 groups when attempting to rebuild the economy. Just one sick group with rampant COVID-19 will bring us all down. Viruses don’t really care about who you are. Celebrity or a jailbird, homeless or a billionaire, it’s all the same to them.
The media has accurately reported how President Trump’s mismanagement of COVID-19 has exacerbated this global health crisis. But Trump’s damage to our public health goes back to the beginning of his administration — and for Congressman Lee Zeldin and the rest of the Republican Party, their culpability starts much earlier.
It begins with the universal Republican vow to eliminate the Affordable Care Act and is compounded by their ideological orthodoxy to starve every federal agency of funding, including those agencies that are charged with public health. Like every Republican, this was the platform Zeldin ran on in 2014, and this is how he has voted as a member of Congress.
But these dual GOP missions — repeal the ACA and reduce the size of government — have directly contributed to the disastrous federal response to this crisis.
The ACA, while primarily concerned with health insurance access and patient protections, also focused on public health issues through the Centers for Disease Control and Prevention. In 2010, the ACA established the Prevention and Public Health Fund (PPHF) at the CDC. It supported a public health mission that included the “early detection of and response to health threats.”
The GOP could not repeal the ACA while Obama was president, but once they took over the House after the 2010 election, largely on the strength of campaigning against the ACA, they worked hard to consistently weaken it, including weakening the PPHF. Then, in 2017, with the inauguration of Trump and complete control of the federal government, they went full-steam ahead to repeal the ACA and reduce the size of all federal agencies. The CDC and the PPHF were no exception.
In early 2018, Trump signed the budget bill that cut the PPHF by $1 billion over 10 years. Later, in 2018, Trump eliminated the global health security office within the National Security Council and made further cuts to public health programs by diverting money from the CDC and the National Institutes of Health for his policy to detain migrant children. Public health experts at the time warned that such drastic moves would harm the country’s ability to respond to and contain outbreaks of disease.
Trump and Zeldin are now working overtime to bury this history. To deflect blame, Trump insists that his name be stamped on the stimulus checks being mailed to desperate Americans. In a similar vein, Zeldin recently announced how he alone got much-needed medical equipment rushed to Suffolk County.
I’m going to start tonight with an important story that slipped under the radar on a day when one outrageous performance after another grabbed headlines.
On its surface, the story doesn’t seem terribly important. A number of congressional committees have asked the Office of Personnel Management for updates on how the OPM is handling working conditions for federal employees during the coronavirus crisis. OPM is declining to answer the requests. “It has always been difficult to get information from this administration, but the refusal to provide Congress with a basic briefing during a pandemic is especially egregious,” said a Democratic Senate aide to Politico reporter Daniel Lippman. “We’ve never been denied a briefing like this before.”
But the story is actually very significant. The OPM oversees the 2 million workers in the federal government. In mid-February, after Republican Senators acquitted him in his impeachment trial, Trump set out to purge the federal workforce of civil servants, whom he sees as “snakes,” and replace them with political appointees loyal to him.
To head the Presidential Personnel Office, which recruits candidates for the executive branch, Trump brought in John McEntee, who had been fired from a former position in the White House by former chief of staff, John Kelly, over a security clearance. On March 17, McEntee forced the director of the Office of Personnel Management, Dale Cabaniss, who had significant personnel experience, to resign. Michael Rigas, formerly of the right-wing Heritage Foundation, took his place. (Phew. I know… but this is going somewhere important.)
The change from Cabaniss to Rigas at the head of OPM transpired just as the novel coronavirus pandemic hit the nation hard.
Rigas has said he believes the 1883 Pendleton Act is unconstitutional. Congress passed the Pendleton Act, also known as the Civil Service Act, after a mentally-ill office seeker shot President James Garfield in 1881. Until then, government positions had been handed out to political loyalists, regardless of their capacity to do the job, but the assassination created a public outcry. Charles Guiteau shot Garfield with the expectation that, once elevated to the presidency, Garfield’s vice president would give Guiteau the position his delusions made him think he deserved. The assassination built momentum behind the idea that government should be non-partisan, and that positions should be filled by people actually equipped to do the job. This sentiment has ruled the nation ever since.
Non-partisan civil service has proved a blessing to the nation in two ways. First of all, over time, as more and more positions came under the act, the government got much more efficient. Second, a non-partisan corps of officials has kept the nation stable since they give their loyalty to the country’s government, rather than to any particular president. Administrations come and go, but government bureaucrats keep the nation on an even keel.
Now, Rigas, the man at the head of the federal government’s 2 million workers, wants to get rid of that system and make all employees of the executive branch political appointees, loyal not to the country but to Trump. Rigas is working with McEntee at the PPO. As of a few weeks ago, agencies now have to submit job openings to the PPO to see if they have anyone they want in the position before they can submit their own choice for it. PPO is filling positions with keen regard for their loyalty: recently it has hired four college seniors to become administration officials.
OPM is the office that is refusing to tell Congress what it’s up to.
Today offered some guesses. Dr. Rick Bright, the director of the Department of Health and Human Services’ Biomedical Advanced Research and Development Authority, or BARDA, claimed that he was let go from his job for crossing Trump. BARDA is charged with protecting us from pandemic influenza and emerging infectious diseases (EID) and Bright is a specialist in those areas. He headed the federal agency developing a coronavirus vaccine, and refused to use the agency’s significant budget to promote hydroxychloroquine, the anti-malarial drug Trump has been pushing as a treatment for the coronavirus. Bright was transferred to a less central position at the National Institutes of Health, but has refused to resign his position at BARDA.
Bright and his lawyers say his removal is retaliation and that he will be filing a whistleblower complaint. “I believe this transfer was in response to my insistence that the government invest the billions of dollars allocated by Congress to address the Covid-19 pandemic into safe and scientifically vetted solutions, and not in drugs, vaccines and other technologies that lack scientific merit,” he said in a statement. “I am speaking out because to combat this deadly virus, science — not politics or cronyism — has to lead the way.”
Bright’s defense of science over politics got a boost with Tuesday’s news that hydroxychloroquine is not only ineffective against Covid-19, but possibly worsens the outcome for those who take it. A study of 368 patients at Veterans Affairs showed that those given the drug were more likely to die than those who weren’t. After much hyping of the drug, Laura Ingraham and other Fox News Channel personalities have suddenly gone quiet on it. Trump, who hailed the drug as a “game-changer” but who has stopped talking about it lately, said he did not know of the bad report, “but we’ll be looking at it.”
Demanding loyalty to Trump is about cementing the power of the president, and service to that power means he will sacrifice his loyalists whenever necessary to protect himself. People are noting that Trump tossed Georgia Governor Brian Kemp under the bus today over Kemp’s reopening of certain Georgia businesses against the advice of public health officials. After a week of calling for states to reopen, Trump told reporters that he “disagree[s] strongly” with Kemp’s decision to start that process.
But Kemp and Trump have clashed before—Trump wanted Kemp to appoint key Trump supporter Doug Collins to the Senate seat that Kemp gave to Kelly Loeffler (now in trouble for insider trading)—so it’s not a huge surprise that Trump hung Kemp out to dry.
Today’s more significant underbussing was that of Alex Azar, the secretary of the Department of Health and Human Services, who was skewered in a piece in the Wall Street Journal for what appears to have been extraordinarily inept handling of the coronavirus crisis. My guess is that he is shortly going to be out of a job, taking the blame for the White House’s poor response to the pandemic.
Considering that Trump’s OPM wants to remove qualified civil servants from the government in favor of political cronies, the piece of the Azar story that has attracted the most outrage is ironic. Azar tapped a key aide with little experience or education in public health, management, or medicine to head up the response of Health and Human Services to the coronavirus crisis.
Before going to work for Azar, the aide, Brian Harrison, was a dog breeder who specialized in labradoodles.
The Republican leader, Mitch McConnell, said yesterday that state and local governments should declare bankruptcy if they find themselves in a financial hole due to the Coronavirus pandemic.
Is he serious?
How in the world do we fight this crisis and bring jobs back if state and local governments are declaring bankruptcy?
Governor Cuomo called out what McConnell said as “offensive”, and “one of the saddest, really dumb comments of all time.” Exactly right.
Mitch McConnell is competing with Donald Trump to be the poster child for demonizing and politicizing a national health crisis.
But what I am really pissed off about is the complete and total silence from Lee Zeldin. Again and again and again, this guy never fights for us. Never!
Even his Republican colleague on Long Island, Peter King said the comments were “shameful and indefensible” and called McConnell the “Marie Antoinette of the Senate.”
But nothing from Zeldin. Nothing.
Nothing but his usual silence in the face of the most extreme in his own party.
Let me be clear, the money the states and local governments are asking for would go to our fire fighters, police officers, EMTs, and healthcare workers.
HEALTHCARE WORKERS! This is who Zeldin will not fight for.
Rt is a key measure of how fast the virus is spreading. It’s the average number of people who become infected by an infected and infectious person. Rt = 1 means one infected person infects one other person on average. If Rt is above 1.0, the virus will spread quickly or logarithmically. For example, if Rt = 2, the progression of infected persons from that one index case goes 1,2,4,8,16,32,64,128,256,…etc. When Rt is below 1.0, the total number of infected persons will start to decrease.
https://rt.live/is a really cool site that tracks the Rt number, by State, and over time.
Here are some examples, but you really should go to the website and look for yourself.
These are the current data for every state in the Union. In green are the states with Rt below 1. In red are the states with Rt above 1:
This was 3 weeks ago:
This is current and highlights the states without stay-at-home (shelter in place) orders:
Rt numbers over time per state:
You can also superimpose these curves with the curves of new cases:
Persistent low Rt numbers as in the case of New York since early April, seems to correlate with “flattening of the curve” of new cases. The reverse also holds true in some states like Ohio where a recent uptick of the Rt number between April 12-19 corresponds with increased numbers of new cases and no flattening of the curve.
I signed up on https://rt.live/ to get updates by email and twitter. I recommend that all those making COVID-19 related decisions, whether nationally or locally, follow these data carefully. They may provide a guide for cautiously reversing stay-at-home orders in some locations.
Please remember: our health and our economy are one and the same.
The 2020 election season moves onward and, across America, people have been asked to either put their health at risk thanks to this pandemic—or not vote.
That’s completely inexcusable. In this time of crisis, we have to protect our health AND protect our democracy.
As New Yorkers, and especially as Long Islanders, we know exactly how important this is.
There is no good reason to delay taking action. Not one.
Voting by mail is safe, secure, and proven. It would allow Americans to exercise their most fundamental democratic rights, all while helping flatten this pandemic’s infection curve by staying home.
This is critical for vulnerable populations – our seniors, Americans with compromised immune systems, workers who have lost their health care – Americans who deserve a voice and a vote, no matter what. Vote-by-mail is also critical for heroes on the front lines – doctors, nurses, biomedical researchers – who shouldn’t be asked to leave work to stand in line at polling places.
Unfortunately, this has become a partisan fight. Donald Trump has even suggested that he’d prefer having fewer voters vote:
“They had levels of voting, that if you ever agreed to it you’d never have a Republican elected in this country again.”
A president of the United States… actually downplaying our civic duty. Unbelievable. And you can bet that Rep. Lee Zeldin is doing nothing to stand up for democracy.
Congress must act immediately to require states to make voting from home easier and to provide the funds to make it happen. In Congress, I will always put democracy first.
I am thinking of you in your little apartment in the epicenter of a global pandemic. I am wishing you good health and safety, and am offering some thoughts on the future and personal empowerment as we look to celebrate Earth Day, April 22, 2020, in the time of Covid.
I was a little younger than you are now on the first Earth Day, 1970. A college freshman then, I was hopeful that a national day would galvanize world collective action to honor our earth: to protect it; to stop polluting it; to bring us all together — my day-to-day life held news reports of the increasing count of body bags coming home from Viet Nam. We had reached an awful peak by then, 54,000 dead, the vast majority my age, 20 and 21. After graduation I moved to New York at a time when my generation faced a recession, high inflation, high unemployment.
So I feel for you, living in this uncertain time, with an uncertain future, marking Earth Day. We are living a different kind of disaster now, fifty years later, one of health. Our nation, and the world, is in shock over a deadly pandemic, and it’s dawning on us that we are all in this together.
The numbers we hear today in the news, as horrible as they are, link directly to our actions. Infections are going down, our Governor Cuomo tells us, because we brought them down. We are all in this together, and we will get through it together.
To me that is hopeful and empowering. I’ve seen wonderful acts of kindness, generosity, our community coming together here on the North Fork, which you know is a virus “hot spot.” Local chefs are making dinners for nurses and doctors, farmers are delivering fresh greens to community food banks, neighbors are calling neighbors to see if they are ok. Thankfully we are all heeding the medical experts and scientists. The infection numbers are down because we are bringing them down.
If you look for it, there are some good news reports: dolphins and swans returning to the canals of Venice, the snowy Himalayasagain visible as pollution drops, white-tailed eagles appearing in England after two centuries. This month in Orient we have witnessed a wealth of young bald eagles.
In honor of Earth Day, I would like to share some hopeful things I’ve learned from Project Drawdown. Both a book and an ongoing climate solutions project, its roadmap for a livable future inspired a group of us to launch Drawdown East End to implement local solutions to reverse the climate crisis.Our first rally last May, at the Southampton Town green attracted about 75 interested people, which has mushroomed into 2,000 wanting to know “what can I do?”
A lot, it turns out. Project Drawdown has identified 80 top “solutions” — opportunities for lifestyle changes that are less polluting, less wasteful, healthier, more economical, that achieve “drawdown” — the point when levels of greenhouse gases stop climbing and begin to come down. The Drawdown book outlines a path for this achievable goal.Actions that can get our lives and economy humming with innovation. Drawdown’s cost benefit analysis shows that starting now to address climate change could save the world $145 trillion.
So, in honor of “we’re all in this together” this Earth Day I’ve pledged to change my life — to align my personal actions with my top 20 Drawdown solutions.* Taking them one by one, making forever changes. Because what I do matters. Because carbon emissions can come down if I (and we, together) bring them down.
I call it my Drawdown lifestyle.
I’m starting with food: Drawdown Solution #3 Reducing Food Waste. It will save me money, it is extremely consequential — avoiding tons and tons of greenhouse gas emissions.
It’s something I can measure, it’s something I can do, it’s empowering. We Americans waste 40% of our food, worldwide it’s over 30%. Cutting that in half would reach Drawdown’s goal for food-emissions reductions. I’m pledging to do better than 50% — to get as close as I can to zero food waste.
“This in an invitation to innovate and effect change, a pathway that awakens creativity,” says Drawdown editor Paul Hawken.
So, right now, our freezer is stuffed, as usual, because I live with a packrat. Mysterious packages from last year, or even before, sit unlabeled. Unlike previous years, my push to “let’s eat from the freezer” has not been met with resistance. Rather, “OK. Good idea.”
Let’s do food the Drawdown way.
Pull out that unmarked package. Get creative. What can we make from this?
Veggie scraps go into freezer bags to later make stock. All leftovers get eaten — for lunch or given new life as a dinner dish. All bones, fish or meat, become stock, or reduced to glaze, to add depth to another creation. The final destination for bones or eggshells is: to the compost (my March birthday present); ultimate destination: enriching the garden.
We are hoping our nearby farmstand will open in May. In the meantime, I’ve joined a local CSA for greens, another one for quail, and have bookmarked this updated list of East End farms open for business. Some send out weekly offerings, which you can order and pay ahead, and pick up curbside. Fresh, local and keeps food-mile emissions down too.
How to reach zero? Use everything. No scraps to the landfill, where they just turn into polluting methane.
Instead, all food is honored, never wasted, any tidbits that remain are tossed into our compost [you can even bury bones (deeply) in your garden.] Composting — Drawdown Solution #60 — is a super solution to me. It’s a win for soil, for farmers, for the climate. Rich carbon soil is created from organic waste, safely sequestering carbon. Spread on farmland, compost increases the capacity of soil to retain carbon (plus aiding water retention and lowering the need for irrigation, fertilizers and pesticides.)
Two more reasons I want to reduce my food waste: 1) rain forests — avoiding their deforestation for additional farmland; 2) methane — avoiding methane-release from landfills, 34 times more powerful than carbon dioxide. Why pollute? Why not consume our food? Why not compost our scraps? Why let any food waste go to a landfill? All this waste.
The U.N. has adopted a planet-wide goal of reducing food waste by 50% by the year 2030.A good article in TIME outlines 4 concrete steps: 1) shop smart, 2) ignore expiration dates—unregulated, set by companies to get you to buy more, 3) divert away from landfills (where 60% ends up) — San Francisco has diverted nearly all its waste from the landfill transforming food waste into compost and selling it back to farmers, 4) transportation spoilage — spoiled while moving food from farm to market, a waste of food, resources, money, which can be corrected.
We now know that we’re all in this together.
And we have an achievable goal: drawdown. Carbon emissions can come down, because we can bring them down, individually, as families, as neighbors, as communities. Want to do something significant for Earth Day? Why not reduce your food waste by 50%?
*P.S. If I piqued your interest: my top 20 solutions are lifestyle changes I can personally make around food, materials, transportation, and energy, as well as community regenerative best practices I can support regarding land and ocean use.
Does Your Kid Have to Wear a Mask Outside? The CDC is asking all adults to wear masks. But what about kids? By Tara Santora Apr 10 2020, 8:25 AM
Why is this question so important? If children were “immune” as suggested by Elon Musk, we could open up the schools and thus free the parents to return to work. It might boost the sagging economy. So goes the reasoning.
Children get infected at the same rates as adults:
“At the beginning of the pandemic, it was thought that children are not getting infected with the coronavirus, but now it is clear that the amount of infection in children is the same as in adults,” explains Andrew Pollard, professor of pediatric infection and immunity at the University of Oxford. “It’s just that when they do get the infection they get much milder symptoms.
This opinion rests on research on people in Shenzhen, China, with confirmed SARS-CoV-2 infections and data from their close contacts:
In total, they looked at 391 people with confirmed COVID-19 and 1,286 individuals who were in close contact.
The researchers’ aim was to find out whether close contacts of people with COVID-19 would test positive for SARS-CoV-2 (the name of the virus that causes the disease COVID-19). And would they transmit virus to their close contacts even when they presented no obvious symptoms?
The investigators found that children under 10 who were in close contact with people who had COVID-19 demonstrated a 7.4% infection rate — very similar to the 7.9%infection rate in adults.
However, the researchers also determined that children were less likely to develop symptoms, even though they seemed just as likely as adults to contract the virus.
The researchers also report that people who lived with individuals who had diagnosed COVID-19 were more likely to develop the infection than other close contacts.
Whereas most COVID-19 cases in children are not severe, serious COVID-19 illness resulting in hospitalization still occurs in this age group. Social distancing and everyday preventive behaviors remain important for all age groups as patients with less serious illness and those without symptoms likely play an important role in disease transmission.
The study describes 1391 children assessed and tested from January 28 through February 26, 2020, a total of 171 (12.3%) were confirmed to have SARS-CoV-2 infection. They conclude: “In contrast with infected adults, most infected children appear to have a milder clinical course. Asymptomatic infections were not uncommon.2 Determination of the transmission potential of these asymptomatic patients is important for guiding the development of measures to control the ongoing pandemic.”
Notes from a pediatrician colleague at Weill Cornell Medicine, Dr. Seth Gordon:
I have found no antibody studies in children. (In case you need a primer on the different types of Coronavirus tests, check here). For the most part, children have been NEGLECTED from the beginning. This has been a tremendous oversight and continues to be a blindspot. Every parent knows children spread infection. They congregate in large groups and are the least hygienic among us. They don’t even make proper masks for children. Children have [likley] been a major vector of COVID-19 spread yet only about 1% of COVID-19 positive tests (RT-PCR swab tests which detect viral RNA) were performed on children. But I believe they represent the vast majority of actual infections. Early on, when I advocated for the closure of schools it was because I was detecting asymptomatic children who were COVID-19 positive. Isn’t this why our schools are closed? I don’t see any evidence that we solved or addressed this issue at all and I see daily evidence of new COVID-19 cases in children. How are we supposed to reassimilate children in schools or camps when we have so little knowledge and testing. It is not even known whether children will develop protective antibodies. This is a HUGE problem in my estimation. While most children do well it is not a universal truth. I have taken care of many sick children during the last two months. As a physician, I feel helpless and frustrated when I can not treat or cure a patient. When Doctor Oz endorses a 2-3% child mortality rate upon returning to school, it really leaves me bewildered as a pediatrician and a parent. If a second wave of COVID-19 comes as predicted, it may be driven by non-immune children in Nov/Dec getting infected and spreading infections to adults again. So it is important to determine the immune status of children BEFORE we return them to school. This way we can make informed decisions.
I would like to add a comment:
If we study the apparent natural resistance in children to the disease (COVID-19), we might gain important knowledge that will help those adults that don’t have that resistance, those that end up in the ICU and on the ventilators. The first step is to test all children, not only adults. Testing and contact tracing is key. It is key to economic recovery too.
For those of us inclined to pay close attention to the Trump administration, this aspect in particular stands out: the undoing of all varieties of federal regulation. Environmental, banking, consumer and health regulations have been targeted for extinction or reduction. In the words of former Trump advisor Steve Bannon, “Our job is the deconstruction of the administrative state.”
Deconstructing important parts of the “administrative state” increases the threats to our health and safety, with loss of life an all-too-common outcome.
Shortly after President Trump was inaugurated, he issued an executive order directing federal agencies to use their administrative powers to begin dismantling the Affordable Care Act “to the maximum extent permitted by law.”
Last July, the federal Centers for Medicare and Medicaid Services, or CMS, proposed a reversal of Obama-era rules that aimed to protect nursing home patients by requiring all nursing home facilities to hire at least one full-time specialist in infection control. Seema Verma, the CMS administrator and a presence at President Trump’s daily coronavirus briefings, expressed concern about not “micromanaging the process.”
It should come as no surprise to learn that a nursing home lobbying group has contributed to the Trump campaign (New York Times, “Regulator Intends to Relax Oversight In Nursing Homes,” March 16, 2020).
The first novel coronavirus hotspot in the United States occurred at the Kirkland Life Care Center for the elderly in Washington State. In neighboring New Jersey, COVID-19 is running through St. Joseph’s Senior Home in Woodbridge Township. And, closer to home, Peconic Landing, an elderly community on the North Fork, is experiencing a heartbreaking toll of infected COVID-19 patients.
Is there a direct cause-effect relationship between regulatory rollback and any one positive COVID-19 case? No, but having a full-time infection control specialist knowledgeable about the science of infectious disease and vector control would have established policy and protocol ready to take the most efficacious approach to life-saving measures.
Mike Anthony
Westhampton
Mr. Anthony is a former Southampton Town Democratic Committee chairman — Ed.
STATEMENT FROM STATE SENATE CANDIDATE DEMOCRAT LAURA AHEARN (SD-1)
Nearly Half of Suffolk County COVID-19 Deaths Occurred at Nursing Homes and Assisted Living Facilities
– Transparency Will Bring Needed Resources –
“On Monday April 13th state health officials released the COVID-19 county-level death toll in assisted living facilities and nursing homes. The coronavirus has killed more than 2,722 people living in such facilities, or about 27% of all virus-related deaths (10,056) statewide as of that date.
According to state health officials, 252 people died at either a nursing home or an assisted living facility in Suffolk County as of Monday April 13th. There were a reported 529 total deaths in Suffolk County as of that date which means that nearly half of all coronavirus deaths in Suffolk County (47.6%) were people living in nursing homes and assisted living facilities.
Our most vulnerable population, our parents and grandparents, are being attacked by a vicious killer and the percentage of deaths in these facilities compared to hospital deaths is disproportionately increasing at an alarming rate. In fact, according to the Governor’s reports, COVID deaths in hospitals and nursing homes on March 20th indicated that 1.4% of overall deaths were occurring in nursing homes but by April 13th that number jumped to 17.1%.
Patient advocates and families with loved ones in these facilities are asking the state to release the total number of deaths and positive cases for each facility across the state. According to Elder Care advocates, disclosure of this information is a public health necessity to raise public awareness so that we can properly gauge the scope of the problem and direct the resources needed to stop the spread and to save lives. Families of loved ones and folks living in these facilities themselves are desperately seeking expansive testing not only of residents but also of staff working there who come and go on a daily basis. If private companies can access testing tools it seems that nursing homes and assisted living facilities who care for our most vulnerable can and should too.
Vaccines are reportedly 12-18 months away, new medical treatments are being explored and discussions are beginning about how to build the bridge to reopen our lives and the economy. Let’s not forget our seniors, one of our most vulnerable populations right now in nursing homes and assisted living facilities that need our immediate help. The very first step is to understand the scope of the problem which begins with releasing the total number of deaths and positive cases for each facility across the state so that policy and lawmakers can direct the appropriate resources to help our most vulnerable.”
Commentary (by D. Posnett MD):
There is no reason for the absence of testing in nursing homes and senior assisted living comunities! Not when there is an ongoing out break in a home like Peconic Landing in Greenport. Not when I can get a test for myself. Not when local physicians in Suffolk are getting tests for their patients. Yes, I know first hand, it is a pain in the neck and may involve hours on the phone or in line at a drive through. But it is feasible.
Why is it important to test everyone at Peconic Landing? They are the largest job provider in Greenport. Some 300-400 people work there and they go home every night to their families. Regardless of whether they work in direct patient care or in the kitchen or on a maintenance crew, they are at risk of bringing the virus out of the facility and spreading it in the community. I am worried about the elderly frail and susceptible residents at Peconic Landing, but I am also concerned about the entire community. Ultimately I am worried about the economic disaster that may follow.
What would we do differently if we had test results? Workers that test positive would have to stay home under strict quarantine, regardless of whether they have symptoms or not (see below). Residents that test negative would have to quarantine, but they might be able to leave the facility after 14 days if symptom free. That is what occurred with passengers on the cruise ships. Workers who develop antibodies (a different kind of test) will likely be safe to return to work, as they may be immune. Finally, we are heading towards massive tracking of positive cases as already done in other countries. Tracking allows one to identify contacts that are in danger of getting the disease. It is useful to start with the origin and in Greenport that would be Peconic Landing.
For every symptomatic person, there are 7 asymptomatic people out there! Note a recent study that just appeared in the New England Journal of Medicine. They tested all women who came in to Labor and Delivery at New York Hospital (Weill Cornell). Only 1.9% (4 patients) had symptoms of COVID-19 and all 4 tested positive by RT-PCR. But 13.5% had NO symptoms and yet tested positive. This means that a lot of people are infectious and spread the disease without even knowing it. That is why EVERYONE NEEDS TO BE TESTED!
In Florida, nursing homes are petitioning the Governor to be shielded from law suits! It sure looks like they are running scared. Perhaps they should be, if they refuse to test when tests are available:
My 3rd ICU Covid-19 patient is not doing well; I can now get testing and millions of unemployed will lose their health insurance.
My third Covid patient ICU patient is not doing well. He is intubated. For the past two weeks I speak to family members every night around 7pm giving them an update. (The ICU staff calls me as I am the primary care physician). Every Covid-19 death is a tragedy; these deaths were largely avoidable. But this patient, who is only 38 year years old, is especially painful for me. I spoke with him the day before he was hospitalized. He called me about symptoms that were likely Covid-19, but he said he was feeling much better. In a familiar Covid-19 scenario, the next day he had trouble breathing, was hospitalized and has been intubated on a ventilator ever since.
I am now able to order Covid-19 tests. Of course, nothing is that simple. There are false negatives. But I do feel that I am making a little progress: yesterday I was able to order the Covid-19 test for someone who had been exposed to the virus and was coming down with symptoms.
By now the (barest) outline of how the United States will emerge out of this totally avoidable human tragedy is becoming clear. The two main questions that remain are.
(1) Will the executive branch of the federal government be held to account for its sheer incompetence, brazen mendacity, and obvious authoritarian tendencies? Will Congress assert its authority and pass significant legislation checking the executive branch? Thus far Congress has been on the sidelines and Fauci is doing a balancing act, And this includes issues like the false hope spread about hydroxychloroquine.
At this time, it also appears that the important recommendations of Scott Gottlieb and Mark McClelland, two excellent health policymakers who served under Republican Presidents, for a strong federal response will not come to pass. States will do their best to respond and many will do just fine; though the political polarization even to Covid-19 will stop for example NY and Florida from working together. (Partisanship, Health Behavior, and Policy Attitudes in the Early Stages of the COVID-19 Pandemic)
(2) Will we, similar to what occurred in the aftermath of the Great Depression, be able to take this unique once in a century opportunity to address the gross inequities in our health system? These will come into sharp relief as millions of people, especially the young, lose their health insurance and are unable to buy it. The Trump administration’s unrelenting opposition to “Obamacare” could become an obstacle for millions of uninsured people in the coronavirus outbreak, as well as many who are losing coverage in the economic shutdown. Health Coverage for the unemployed will be harder to come by in some states.
It is not just the young but as we already know, Covid-19 discriminates: the “pre-existing health conditions” that put a person at risk of severe disease and death from COVID-19 are over-represented in communities of color and poor communities as a result of long-term disinvestment and neglect.
The answers to this “once in a century opportunity” are completely dependent on citizen group mobilization and the extent to which groups such as the hospital industry, health professionals small business groups and unions see it in their interest to collaborate.
‘Ask Nurses and Doctors’ (AND) is doing its part by working with health professionals in competitive Congressional districts organizing for election of incumbents and/or candidates who prioritize universal coverage; we are also organizing in swing states such as Florida and Michigan to help elect a Democratic President. This once in a century opportunity is dependent on policymakers coming up with feasible ideas that can be quickly implemented. Akin to what the states of Mass. and Washington are doing. In essence, the initiatives use traditional public health measures for a debilitated public health system. I will summarize what I and other colleagues are calling Community Centered Population Health (CCPH) – as our response to this once in a century opportunity. CCPH is community centered (not patient centered) health care that links public and personal health with community health workers as the first line.
Long Island needs a leader right now, not a rubber stamp for the Trump administration’s irresponsible policies and erratic procedures. That’s not how a member of Congress should act.
Congressional District NY-01 in Suffolk County should have a representative who will demand fairness for his residents. Instead, we have Lee Zeldin, who is too busy covering for Donald Trump’s antics and failure to respond responsibly to this crisis.
Recently, Congress passed a 3rd stimulus package with support from both parties. But guess what? New York State got short-changed and Zeldin did nothing, despite two important facts:
Our state has suffered more than any other state from the pandemic with 35% of confirmed Coronavirus cases and 42% of all the deaths in the US. The Trump administration has ignored our plight and decided to allocate hospital aid based on old data, instead of basing it on the number of Coronavirus cases. This decision will bankrupt our hospitals and leave healthcare workers to do without. It is a slap in the face to our heroes on the frontlines.
New Yorkers have the highest costs of living nationally, particularly in the New York Metro region. Yet we face the same financial criteria for direct cash payments as people from other parts of the country with a much lower cost of living.
These two problems that New Yorkers are facing must be addressed in the next stimulus package. Lee Zeldin should be doing everything in his power to make sure that our state gets the relief it needs. But he won’t. Instead, he will just raise his hand and vote however the leadership in his party tells him to. That’s unacceptable. A good member of Congress should fight for his constituents.
In Italy, men made up nearly 60 percent of people with confirmed cases of the coronavirus and more than 70 percent of those who died of COVID-19. In China men and women were infected in roughly equal numbers, but the death rate among men was 2.8 percent, compared with 1.7 percent among women. The same applies to South Korea and numerous other countries. In New York City, men are dying at nearly twice the rate of women. As of recently, men made up 59 percent of overall hospitalizations in New York City and 62 percent of fatalities. In 13 states with sufficient death numbers for analysis, men died more frequently than women.
Men were also disproportionately affected by SARS and MERS, caused by related, but different coronaviruses. For SARS, in Hong Kong in 2003, the case-fatality ratio was 13.2 % for women and 22.3 % for men. Also, 32% of men with Middle East Respiratory Syndrome (MERS) died, compared with 25.8% of women.
The question is: Why?
At first, risk factors were blamed. For instance, smoking rates among men exceed those among women in much of the world. 2% of Chinese women smoke, compared with more than 50% of Chinese men.
Chinese men also have higher rates of Type 2 diabetes and high blood pressure than Chinese women, both of which increase the risk of complications following infection with the coronavirus causing COVID-19 (SARS Cov2). Rates of chronic obstructive pulmonary disease are almost twice as high among Chinese men as among women.
Women are more proactive about seeking health care than men. Since the start of the outbreak, public health officials have emphasized the importance of washing hands to prevent infection. But studies have found that men — even health care workers — are less likely to wash their hands or to use soap than women. While these 2 considerations might affect the number of diagnoses made and perhaps the rate of hospitalization, they are unlikely to affect mortality in my view.
Moreover, rates of smoking in the US are quite similar comparing men to women (unlike in China): in 2015, 16.7 percent of adult males and 13.6 percent of adult females smoked cigarettes in US. Yet the death rate from COVID-19 is clearly much higher among US men compared to US women.
Let’s consider biological differences. Women have more robust immune systems, some scientists have noted, which helps to fight off infections, although it does make them more prone to autoimmune disorders.
When it comes to mounting an immune response against infections, men are apparently the weaker sex. “This is a pattern we’ve seen with many viral infections of the respiratory tract — men can have worse outcomes,” says Sabra Klein PhD, a scientist who studies sex differences in viral infections and vaccination responses at the Johns Hopkins Bloomberg School of Public Health.
Says Dr. Klein: “We’ve seen this with other viruses. Women fight them off better. Women also produce stronger immune responses after vaccinations, and have enhanced memory immune responses.”
A recent research paper from Huazhong University of Science and Technology in Wuhan, using plasma of 331 confirmed coronavirus patients, found that in the most severe cases, women had higher levels of antibodies than men.
For almost all infectious diseases, women are able to mount a stronger immune response then men. Women with acute HIV infections have 40 percent less viral genetic material in their blood than men. Women are less susceptible to the viruses that cause hepatitis B and C. Men infected with coxsackie virus (which can infect the heart) are twice as likely to die of the disease than women.
Female birds show higher antibody responses to infection than males, especially during mating season. The immune cells that eat up microbes and cellular debris are less active in male lizards than in their female counterparts.
Some 60 genes involved in immune function are located on the X chromosome (according to Dr. Sabra Klein). Genetic females have two of these molecules — one from their mother, one from their father — whereas genetic males have only one. When there are two copies of a gene, one copy is often turned off. But as many as a quarter of X-linked genes can escape this inactivation, giving women a “double dosage” of the genetic instructions needed to fight disease.
One such gene codes for a protein called “toll-like receptor 7,” This receptor recognizes strands of viral RNA (the Coronavirus is an RNA virus)
Generally, female immune cells respond faster and more powerfully to viral attacks, producing higher amounts of interferons — proteins that stop viruses from replicating — as well as antibodies that neutralize the virus
Testosterone, has been shown to tamp down inflammation. Estrogen, meanwhile, can bind to immune cells and activate the production of disease-fighting molecules.
A recent study demonstrates a direct role for estrogen signaling in limiting influenza virus replication in nasal epithelial cells derived from humans
ACE2 is a receptor for SARS Cov2. It allows the virus to gain access and infect cells. ACE2 is regulated differently in men and in women.
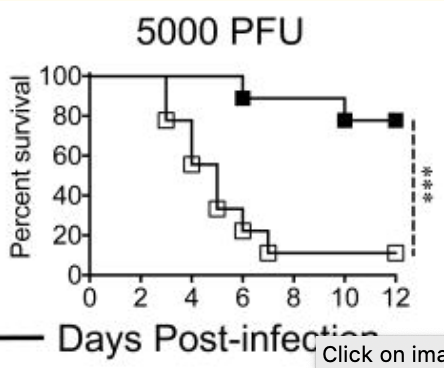
Experiments published in 2017, in which mice were exposed to the SARS virus (SARS Cov), showed that male mice developed SARS at lower viral exposures, had a lower immune response and were slower to clear the virus from their bodies. They suffered more lung damage and died at higher rates – see the graph below! When researchers blocked estrogen in the infected female mice or removed their ovaries, they were more likely to die, but blocking testosterone in male mice made no difference, indicating that estrogen may play a protective role.
Solid squares are female mice; open squares are male mice. 12 days after infection, 80% of female mice and only 10% of male mice were still alive. 5000 PFU is the dose of virus used to infect each mouse (PFU = Plaque Forming Unit)
Despite all of this, the coronavirus vaccine trials underway in the U.S. aren’t really considering sex yet, according to Dr. Klein. If past experience holds up, vaccines will be more effective in women than in men!
STATEMENT FROM STATE SENATE CANDIDATE DEMOCRAT LAURA AHEARN (SD-1)
“The first 30 billion dollar distribution of federal coronavirus aid for hospitals is not being allocated based upon the incidence of COVID-19, but instead upon the number of Medicare recipients in 2019.
The use of this formula is disastrous as New York State and Long Island, the epicenter of the pandemic in the US, are slotted to receive minimal funding, far below what is desperately needed as our state and local governments attempt to manage this human catastrophe.
New York currently has 35% of the cases nationwide and is getting just 6% of the $30 million being distributed. According to Newsday, New York will receive $1.86 billion — less than the $2.9 billion for California with only 4% of the cases, $2.2 billion for Florida with only 3.6% of the cases, and $2.1 billion for Texas with only 2.2% of the cases.
State
% of all COVID cases
Billion
as % of 30 billion total aid
New York
35.0%
1.86
6.2%
California
4.0%
2.9
9.7%
Florida
3.6%
2.2
7.3%
Texas
2.2%
2.1
7.0%
I strongly urge all of our Federal Representatives to stand up and fight to ensure that any additional federal aid is geared towards communities hardest hit and in the most need, like ours. For decades, New York residents have paid more in federal taxes than what we get back in return. Now is the time for Washington DC to be there for New Yorkers.”
By Laura Ahearn
Comment by D. Posnett: New York State is being ripped off and representatives, like Congressman Zeldin, will bear responsibility if this does not change.
I am not sure why, but for the first time, each day this past week found me on multiple Zoom conference calls. Each of these was for a different group that I belong to, from my local Southampton Democratic Club to the national grassroots women’s group, SuperMajority. It is as if we all collectively woke up to the reality that this lockdown is going to be a long haul and this is the new normal not just for a few weeks but for a few months.
Like everyone, I am shaky with anxiety over this pandemic, worried that the people I know and love could become a statistic of this disease. I live in the suburbs outside of New York City where we have our own rising cases, though nothing like the five boroughs of the city. I lived on the Upper West Side of Manhattan for 25 years and my heart is breaking for what I will always consider “my city.” But my worst, chest-tightening moments of panic come when I think of my family members who are nurses on the front lines of this crisis. How can it be that in the United States, a healthcare provider is now taking his or her life in their hands just going to work? Every single one of these heroes deserves more than thanks from a grateful nation, they deserve wartime hazardous duty-pay. In lieu of that, the least this government can do is have their student debt wiped off the books for the job they are doing, risking their lives to save ours. We need to all start a movement to make this a reality. What would be a great hashtag for this mission, #thanksarenotenough?
Two weeks ago my anxiety reached a maximum level when my husband, son and I all came down with a cold. How surreal that the common cold induced frantic days obsessively taking my temperature and sleepless nights of pure dread, kept awake by coughing that I could not determine if it was wet or dry. It was hard to get through to the primary care physician’s office, the line was always busy, but once I did speak to a nurse my question was, “at what point should we worry?” Since there was no fever, chills or shortness of breath, she told me it was probably exactly what it appeared to be, a simple cold, but if any of those three symptoms appeared, to call right back. Call right back, I thought? It took me hours to get through this time when I didn’t have fever, chills and shortness of breath. But each day the cold lessened and by week’s end had passed as colds are wont to do. But this simple cold left a residue of fear in its wake that made me reluctant to even go outside for a socially-distant walk.
So, I have asked myself if in the midst of this once-in-a-century public health and economic crisis, should I take a break from politics, if only to help maintain my sanity? On our Democratic Club call the focus was on how can we reach out and help those in our township who are really suffering because they can no longer afford to buy food. It felt good to be helping out with something that was not political. I also gave up watching my MSNBC line-up at night. I listen to music while riding my exercise bike rather than watching Rachel Maddow. Some nights we watch movies, particularly movies that make us laugh. I still read the newspaper each morning but I skim through a lot and I have tried not reading headlines on my phone all day. It has helped quiet some of the panic.
But even digesting a much lighter diet of news, I cannot escape one undeniable fact, that this crisis, all of it, from the number of infected and dead, to the dire shortage of personal protective equipment for our healthcare providers, to the shuttering of businesses and skyrocketing unemployment, to the food shortages for low-income families, every bit of this trauma the country is now enduring, has been made much worse by the incompetence, selfishness and corruption of the Trump administration. And this inescapable fact sits in the pit of my stomach and emits a rage so white-hot that I can’t ignore it. And because of that, I can’t stop worrying about politics and in particular, the election this fall.
The Washington Post put together a complete accounting of just how much of a mess the Trump administration has made of our preparedness for this crisis. The April 4th article is entitled “The U.S. was beset by denial and dysfunction as the coronavirus raged: From the Oval Office to the CDC, political and institutional failures cascaded through the system and opportunities to mitigate the pandemic were lost.” It is a big, investigative deep-dive into the dysfunction. It is gut-wrenching and infuriating but maybe the most important article every single American needs to read.
On March 30th the Editorial Board of The Boston Globe, put the blame for this failure of leadership squarely where it belongs. The title of the editorial says it all: “A President Unfit for a Pandemic. Much of the Suffering and Death Coming was Preventable. The President Has Blood on His Hands.”
To quote the editorial: “As the American public braces itself for the worst of this crisis, it’s worth remembering that the reach of the virus here is not attributable to an act of God or a foreign invasion, but a colossal failure of leadership.”
Much like The Washington Post article, the editorial goes through the entire timeline of failure on the part of the Trump administration and ends with the statement, “But come November, there must be a reckoning for the lives lost, and for the vast, avoidable suffering about to ensue under the president’s watch.”
It is this need for a reckoning that mandates we stay focused on politics and keep our eyes on the November election, despite the pandemic that rages around us. When Trump was elected, our outrage sparked the Women’s March and created the anti-Trump Resistance. That movement powered the blue wave in 2018. Despite the fears that now haunt our days and plague our nights, we must not lose sight of what has always been our prime directive, to make sure Trump is a one-term president. Our work in the Resistance was how we channeled our rage then and it must be how we channel our rage now.
But unlike the last three years, we cannot organize and attend rallies, we cannot knock on doors and speak directly to voters, we cannot even be together in a planning meeting or a Happy Hour social event. All last week, on every Zoom call with every organization, we struggled to answer the same question, “How are we going to get the public engaged when we are stuck in our homes?”
In an article on, April 5th, The New York Times addressed this dilemma from a campaign’s point of view. “With Campaigns in Remote Mode, Pandemic Upends Battle for Congress: As retail campaigning has become all but impossible amid the public health crisis, candidates tread carefully in an uncertain political environment.”
This article did not address the dilemma from the non-candidate point of view, meaning how are we in the grassroots going to function this year if we cannot go outside? The next day, April 6th, The New York Times corrected that oversight with an article looking at the impact on progressive campaigns and on the grassroots movement from the pandemic. “Progressives Built an Organizing Juggernaut for 2020. Then the Virus Hit: After a disappointing turn in the presidential race, grass-roots progressive groups focused on congressional races and down-ballot campaigns. In weeks, the coronavirus has destroyed their plans.”
To quote from that article: “The grim picture may have a profound political impact for the general election and beyond. Democrats were poised to have an organizing juggernaut ready for the 2020 election, with the goal of both reaching new voters and helping reverse the state and local losses they experienced during President Barack Obama’s years in power. Even more, liberal groups hoped this election cycle would formalize their political infrastructure, so the activism that erupted in response to Mr. Trump’s election could be harnessed going forward. That may still happen, but it will require creative financial and digital solutions, according to interviews with several leaders of progressive political organizations and left-wing candidates running for office in states like New York and Ohio. Optimists have called it a time for political innovation, while others worry the structural barriers could stymie the progressive movement at a critical crossroads.”
The article zeroed in on the bind we are all in. We spent 2017 learning how to get out of our houses and speak in person to voters. Then in 2018 we utilized that knowledge and those skills to propel the largest voter turnout for a midterm election in 40 years. Now we have to learn how we are going to be effective without person-to-person contact.
Below are a few initiatives that are trying to address that need. The first is an app called Outvote that is mentioned in this article. Here is the description on their website: “Outvote is an app that makes it easy to support the causes and campaigns you care about. The goal of the app is to promote voter participation within progressive campaigns. Our larger mission is to build a community of organizers that remain active between election cycles. By partnering with the biggest campaigns, advocacy organizations, and nonprofits, the Outvote community will be able to mobilize around current events, elections, and critical moments in policy formation for social equality and justice.” https://www.outvote.io/
But Outvote seems to be primarily for organizers, a valuable resource but not really a direct conduit to voters. Indivisible has an ongoing project with a direct line to voters that activists can participate in from their homes. It is called VoteFWD and involves writing letters to voters in swing states. Here is the description from the Indivisible website: ‘Want to get out the vote in key states from the comfort of your own home?Indivisible is excited to be partnering this election cycle with VoteFWD. VoteFWD provides activists with names, addresses and a data-driven proven template to write letters to voters in important states. Letter writers will save their letters and send them right before the election so that voters receive them at the perfect, most-strategic moment.”https://indivisible.org/resource/write-letters-voters-votefwd
On my Zoom call with SuperMajority, which joined with Pantsuit Nation, I heard about two projects. The first is called Turnout Tuesday where they are asking their members to call their state Secretaries of State and press them on how they are going to use the federal funds to make sure the vote in November is secure, particularly if they are going to invest in mail-in ballots. The second is text messaging to voters and they have been conducting training seminars to teach members how to do “rapid response textbanking” to alert voters about important issues. https://supermajority.com/
At my local Indivisible group, East End Action Network (EEAN), we were already planning postcard-writing parties, creating and mailing personal postcards to voters in our district, as we did in 2018. This will be a joint project with Indivisible North Fork. These events will begin in July, after the New York primary on June 23rd when we have a Democratic congressional nominee. While it is certainly more fun to party together (you can read the descriptions of these events in my book, The Resistance and Me, available on Amazon), we can convert this initiative to home-based postcard writing rather than in groups if we are still not able to gather together by the summer. The end goal of getting the postcards out there can still be achieved.
These are all good ideas. But they don’t go far enough. The voter suppression outrage by the GOP in Wisconsin underscores the extreme lengths the Republicans will go to keep people from voting. We are going to need bigger and bolder ideas to take the place of speaking to voters in person if we are going to be able to counter those GOP schemes. Possibly because they are aware of this challenge, Indivisible will be hosting a series of training webinars in April for Indivisible leadership on how to better use the virtual space during this lockdown period. If you are a member of an Indivisible group, someone in your leadership has probably already received an email about signing up. If not, reach out to your Indivisible contact. I tried to find a link for these webinars on their general website and could not find one. I look forward to whatever ideas come out of these webinars and will include them in later blog posts.
I am particularly worried what happens to voter registration. Normally the spring and early summer are key periods to focus on voter registration but how can that be done digitally and from our homes? I have been wondering if it is at all possible to conduct a virtual voter-registration drive and I would love to hear back if anyone has any ideas about this. How can we reach residents in the district who are not registered to vote? Is that even possible? They wouldn’t be in MiniVAN but would there be a way to cross reference residents with voter registration rolls to determine constituents who aren’t registered? We could mail them personal letters including the voter registration form if they cannot register online through the state motor vehicle department. Is there any way at all we could create such a list?
Along with my fear that we are not going to be able to register new voters, is a concern that our digital efforts are not going to reach the Independents and Unaffiliated voters we need to win in November. Maybe we should think about sending postcards right now to these voters with the facts about how the Trump administration has mishandled the pandemic, facts that would break through the fog of misinformation that Trump and his propaganda machine at Fox News are spewing out. These postcards could also have contact information for services that many constituents need during this crisis, such as food banks and how to file for unemployment benefits. And these voters are in MiniVAN. We would have to figure out how to pay for printing the postcards and the postage since these would not be funded by the campaigns.
We know from the midterm election how much time, effort and boots on the ground it took to power the blue wave. It is a process that starts months before with voter registration, educating the public, supporting primary candidates and then getting-out-the-vote. We do not have the luxury of waiting for the crisis to pass, waiting until we are able to knock on voters’ doors, not while Trump and the right-wing media saturate the airwaves with lies about this pandemic while at the same time erecting barriers to voting. If we are going to hold Trump and the GOP accountable in November, we need to act now and to do that we need bigger and bolder ideas of how we are going to reach voters, counter the lies and protect the ability for every American to vote.
By Barbara Weber-Floyd
Author, The Resistance and Me: An Insider’s Account of the Two-Year Mission to Stop the Trump Agenda and Take Back the House
(Available on Amazon and at Canio’s Books, Sag Harbor)
There has been talk about the flattening of the curve of new reported COVID-19 cases indicating at the very least a slowing growth of the caseload in New York City. I found the following data in an interesting “working paper” by Jeffrey E. Harris from the National Bureau of Economic Research: The Coronavirus Epidemic Curve is AlreadyFlattening in New York City. It was posted April 7th. Others have also opined on the same topic: Joseph Goldstein in the NY Times; Bob Herman on Axios.
Here is a brief summary of the Harris paper.
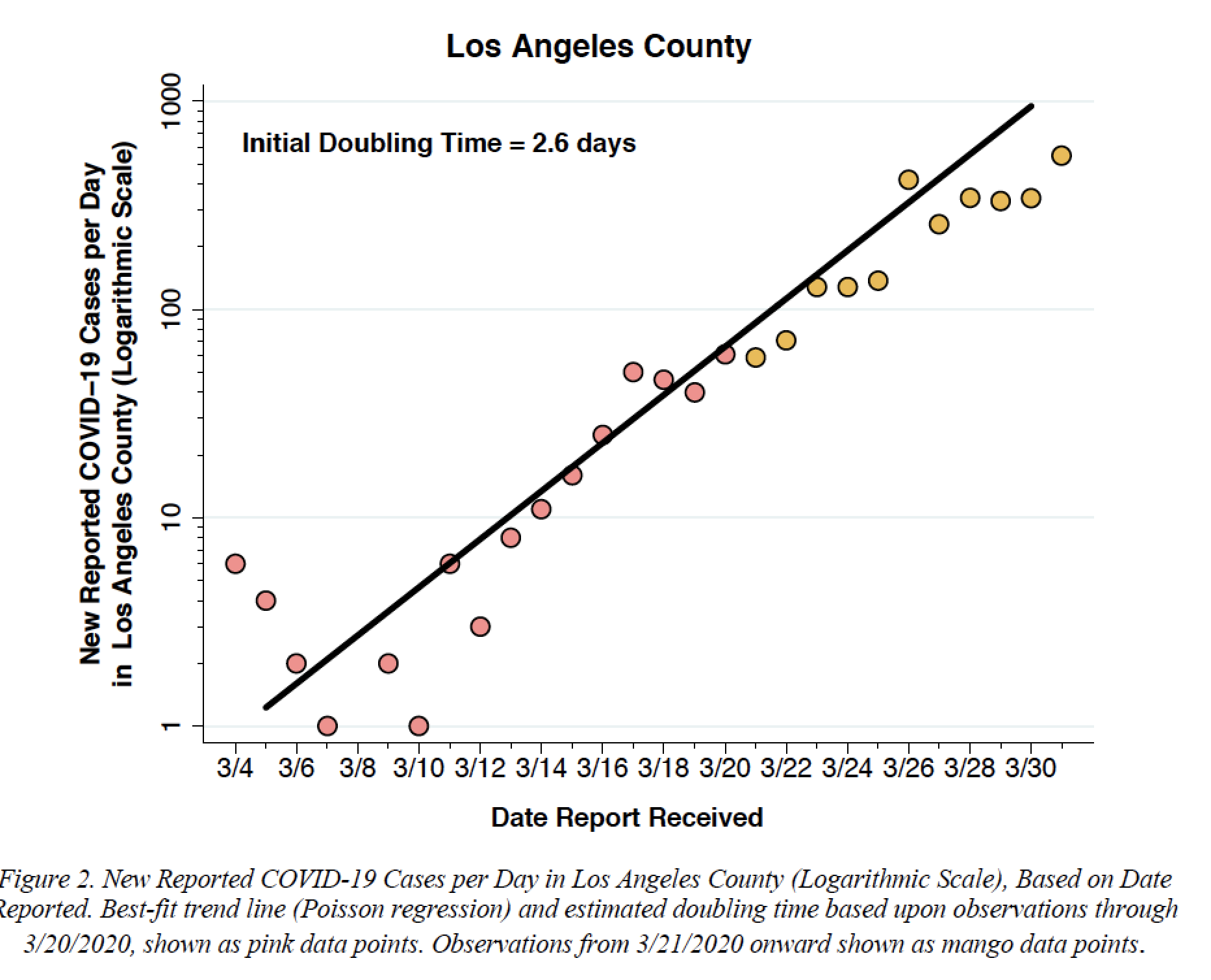
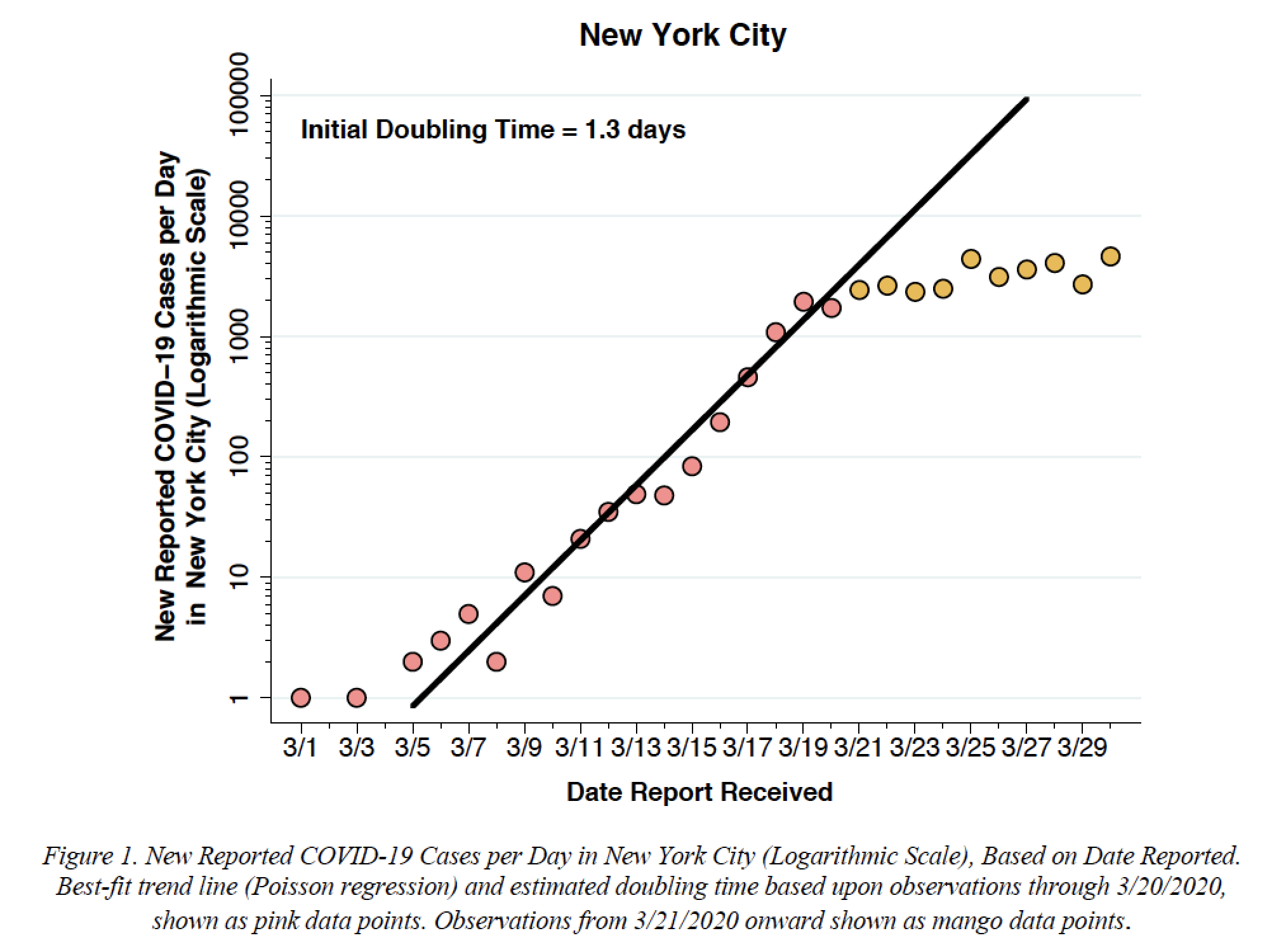
Note the inflection of the curve of new reported cases/day around March 20, 2020, in NYC but not in Los Angeles. Also note the different case numbers: Y-axis 1-1000 for LA, 1-100,000 for NYC. Most certainly the situation in LA reflects an earlier time point in the progression of the local Coronavirus outbreak. NYC may be an indicator of what is yet to come in LA.
The most valuable part of the Harris paper (I think) is the discussion of the possible confounding variables.
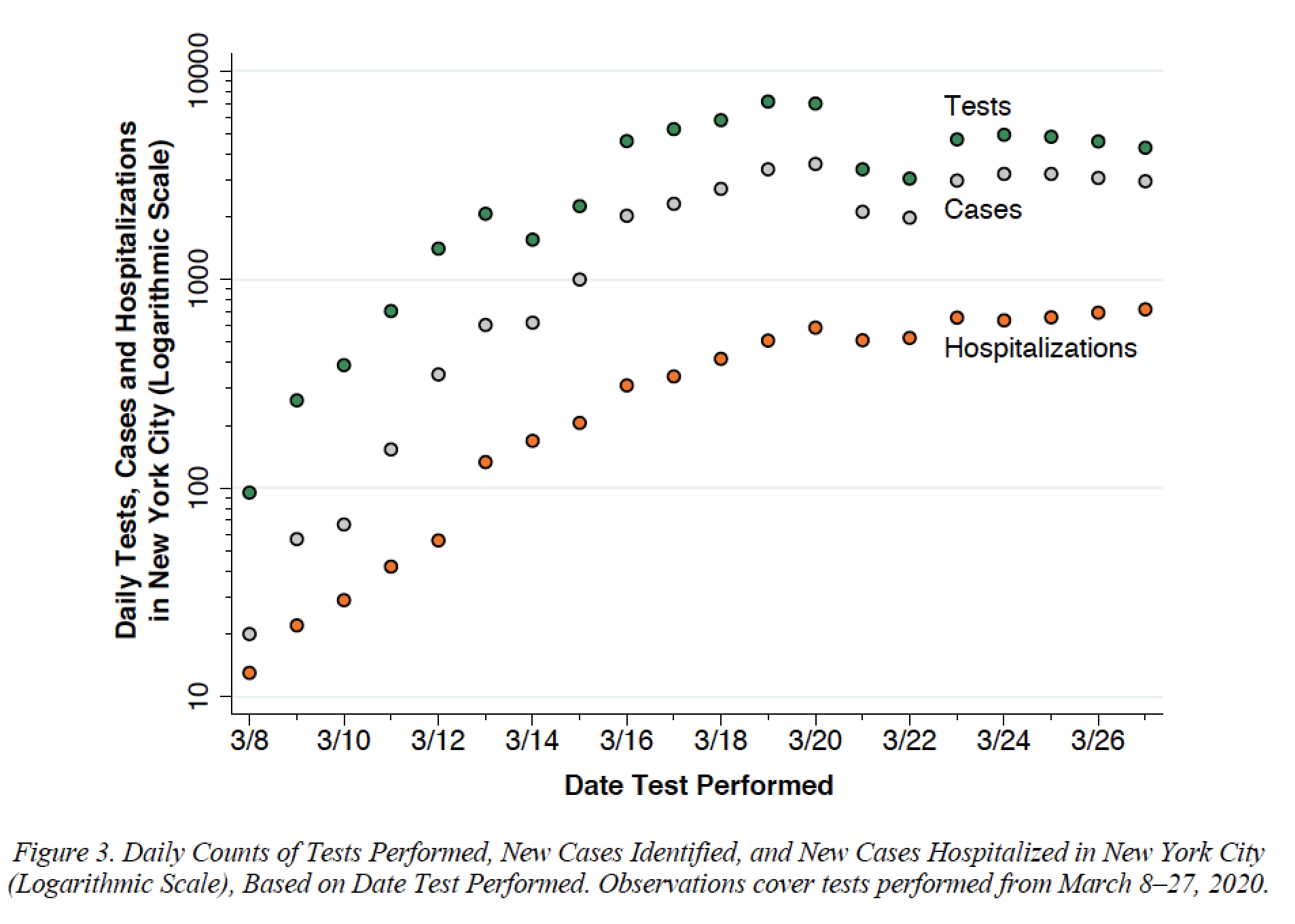
(1) Constraints on Testing: on March 20 New York City issued a directive “Healthcare resources must be saved to treat the sickest patients who require inpatient and critical care.” The Department directed providers and hospitals to “immediately stop testing non-hospitalized patients for COVID-19 unless test results will impact the clinical management of the patient. In addition, do not test asymptomatic people, including HCWs [healthcare workers] or first responders.”
In deed there was an immediate dip in the number of tests by about 50% and a simultaneous dip in the number of reported cases by about 30%. But the dip in hospitalizations was much less prominent (about 10%) and they provide further data that show that the tests performed on hospitalized patients remained constant at about 17-23% of all tests performed:
Note: the Y axis is a logarithmic scale.
(2) Asymptomatic cases not considered: as many as 50% of COVID-19 cases may be asymptomatic and untested, yet infectious and contributing to the rise in the counts of newly diagnosed each day. But Harris argues: “…there is no clear reason to believe
that the extent of understatement has changed significantly since the one-month takeoff period covered in Figure 1. So long as the ratio of undetected asymptomatic cases to detected symptomatic cases has remained constant”
(3) We are missing the false negatives: tests based on nasal swabs (RT-PCR tests) have a false negative rate in the range of 26.7–46.4% (Yang et al. 2020). That means routine nasal swab testing could be missing a lot of coronavirus infections. But has the percentage of false negatives changed significantly during the month of March 2020 to explain the flattening of the curve in NY City?
(4) What is the breakdown of the data by borough: There are reports of hospitals in Queens and the Bronx being overwhelmed and a heat map from the Dep. of Public Health, shows high levels of pos. tests in the Bronx, Queens and Brooklyn. Harris presents data on new cases since March 21 broken down by borough. All the doubling times remain longer than the initial 1.3 days doubling time in early March, regardless of the borough. But the data for Manhattan are particularly good suggesting a flattened peak and leveling off.
(5) Diaspora from the city: assuming that those that fled the city (for their Hamptons 2nd homes, for example) have equal rates of infection than those that did not or could not, Harris has calculated that 90% of the New York City’s inhabitants would have needed to flee the city in order to cause the flattening of the curve in the top figure.
(6) Is the initial rapid progression realistic? The Ro number (‘basic reproductive number’, or number of people infected by one positive person) differs slightly depending on the city:
New York City: Ro=3.4 population density 27,016/square mile
Los Angeles: Ro=1.8 population density 7,544/square mile
Wuhan: Ro =2.2 -2.4 population density 3,200/square mile
This is most consistent with the high population density in NYC compared with LA, or even Wuhan. Population density in NYC has previously been discussed in the context of the pandemic. This is the most plausible cause of the rapid progression observed in New York City.
(7) Super-Spreaders: this theory suggests that the apparent flattening of the incidence curve is a result of extreme heterogeneity in the infectivity of the New York City
population, with a small proportion of the total population – on the order of 5,000 individuals – subject to the super-spread of the virus. While there are anecdotal reports of such super-spread in the New York City area (Williamson and Hussey 2020), Harris has not found clear evidence of a major source comparable to the 77 COVID-19 cases reportedly emanating from a late February Biogen meeting.
(8) Supporting Ancillary Data? Harris correctly discusses daily death rates as a poor and lagging indicator. By one estimate, it takes an average of 16 days from the onset of symptoms until a patient dies of complications and the time from initial
infection to death may average about 3 weeks. Harris also looks at thermometer data from Kinsa! I have previously posted on this blog about this exciting new way of assessing pandemic progression.
The downward slope of the red line is interpreted as a resolution of the Coronavirus outbreak. BUT it is very indirect data and there is no data presented for Los Angeles !!! Why not? If Harris is correct there should be no downward slope for Los Angeles.
In asking what makes the curve flatten, Harris discusses the obvious: social distancing, aggressive case tracking and effective public policy such as De Blasio’s order limiting gatherings, closing gyms and other places of congregation and reinforced by subsequent orders that all New Yorkers (except workers in essential businesses) must stay at home.
The discussion of voluntary behaviors is very relevant. Ridership on New
York City subways was already down 19 percent by March 12 and 60 percent by March 16 (Metropolitan Transportation Authority 2020).
The critical ingredient in the public policy mix may have been the successful communication of consistent, clear, accurate and timely information to millions of individuals, who responded by taking action without government coercion. Put bluntly, what flattened the curve was no more than the naked truth.
Finally, in NY City about 1/226 residents have so far contracted COVID-19. In Los Angeles, by contrast, it is about 1/4,100. The corresponding probability of knowing at least one infected person in a comparable size social circle is much less in L.A. than in NYC. People are therefore more motivated to take action to reduce risk in New York.
They analyzed levels of 48 cytokines (!) in COVID-19 patients and healthy controls.
Key Findings:
• Many cytokines were elevated with COVID-19
(IFNy, IL-1Ra, IL-2Ra, IL-6, IL-10, IL-18, HGF, MCP-3, MIG, M-CSF, G-CSF, MIG-1a, and IP-10). IP-10, IL-1Ra, and MCP-3 (esp. together) were associated with disease severity and fatal outcome.
• IP-10 was correlated to patient viral load (r=0.3006, p=0.0075).
• IP-10, IL-1Ra, and MCP-3 were correlated to loss of lung function (PaO2/FaO2 (arterial/atmospheric O2) and Murray Score (lung injury) with MCP-3 being the most correlated (r=0.4104 p<0.0001 and r=0.5107 p<0.0001 respectively).
• Viral load (Lower Ct Value from qRT-PCR) was associated with upregulated IP-10 only (not IL-1Ra or MCP-3) and was mildly correlated with decreased lung function: PaO2/FaO2 (arterial/atmospheric O2) and Murray Score (lung injury).
• Lymphopenia (decreased CD4 and CD8 T cells) and increased neutrophil correlated w/ severe patients.
Caution: Collection time of clinical data and lab results was not reported directly making it very difficult to determine if cytokines were predictive of patient outcome or reflective of patient compensatory immune response. Small numbers for cytokine analysis (N=2 fatal and N=5 severe/critical, and N=7 moderate or discharged). @sinaiimmunologyreviewproject
What is IP-10? Also known as CXCL10: it is a chemoattractant for various types of white blood cells and promotes inflammation.
What is IL-1Ra? The interleukin-1 receptor antagonist (IL-1Ra) blocks the IL-1 receptor and is a natural inhibitor of the pro-inflammatory effect of IL1 (which causes fever for example). A slightly modified version of IL-1Ra, called anakinra, is used in the treatment of rheumatoid arthritis, an autoimmune disease in which IL-1 plays a key role
What is MCP-3? Also known as CCL7. It is a chemokine that attracts monocytes, a type of white blood cell.
It is beginning to look like a familiar scenario. Too much of an immune response is not a good thing. Cytokine storms have famously contributed to the lethality of influenza such as the Spanish flu of 1918.
It may be premature, but it is the best available data to explain why some with COVID-19 have a minor disease and others have life threatening disease.







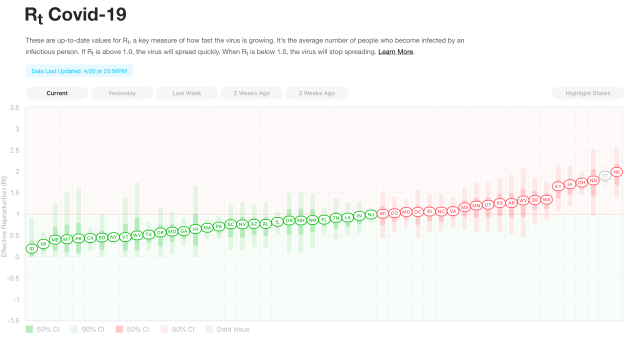
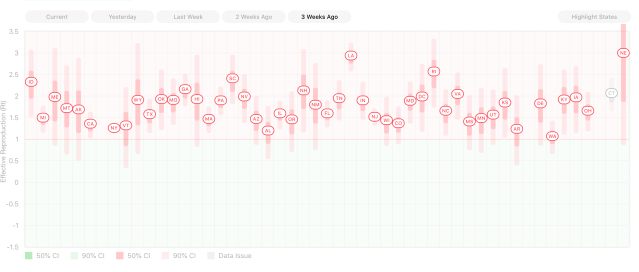
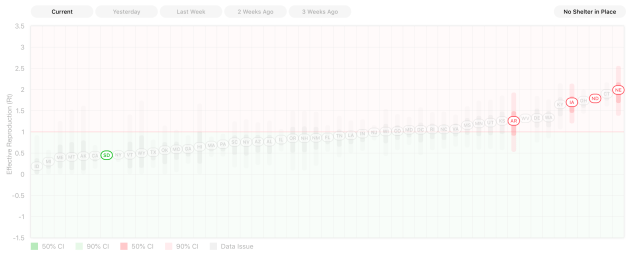
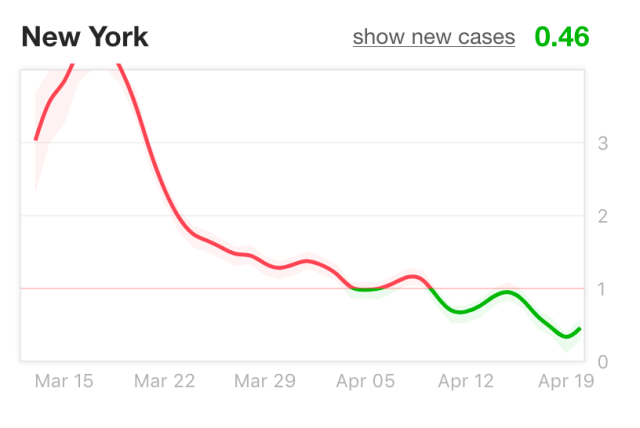
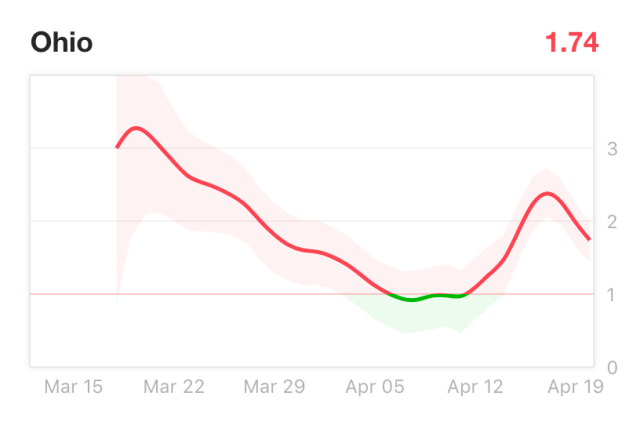
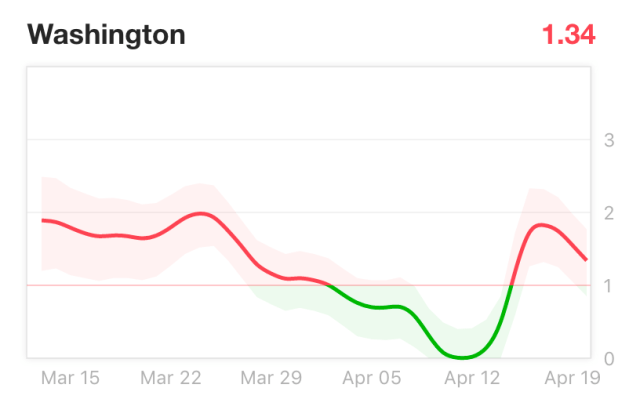
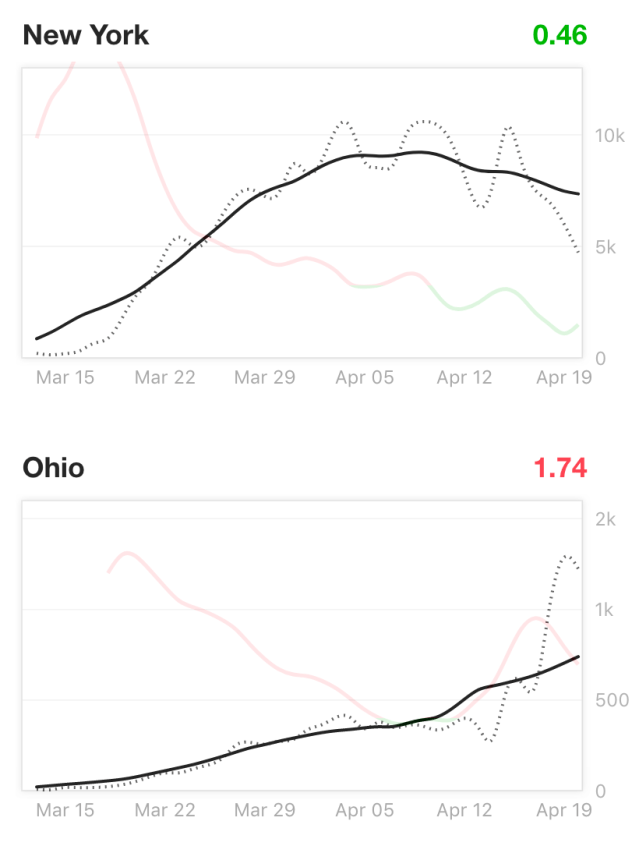



 In honor of Earth Day, I would like to share some hopeful things I’ve learned from
In honor of Earth Day, I would like to share some hopeful things I’ve learned from