Click and watch this disturbing video from a Bergamo hospital
Click and watch this disturbing video from a Bergamo hospital
A new report published by the New England Journal of Medicine (NEJM; arguably the top medical journal in the world) makes the point that hospitals are major sites of corona-virus transmission and home care (community-centered care) would be a better model. It is also a dramatic plea for help.
March 21, 2020.
In a Bergamo hospital deeply strained by the Covid-19 pandemic, exhausted clinicians reflect on how to prepare for the next outbreak.
Summary
In a pandemic, patient-centered care is inadequate and must be replaced by community-centered care. Solutions for Covid-19 are required for the entire population, not only for hospitals. The catastrophe unfolding in wealthy Lombardy could happen anywhere. Clinicians at a hospital at the epicenter call for a long-term plan for the next pandemic.
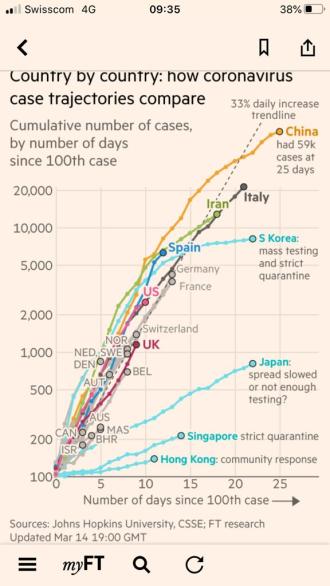
We work at the Papa Giovanni XXIII Hospital in Bergamo, a brand-new state-of-the-art facility with 48 intensive-care beds. Despite being a relatively small city, this is the epicenter of the Italian epidemic, listing 4,305 cases at this moment — more than Milan or anywhere else in the country (Figure 1). Lombardy is one of the richest and most densely populated regions in Europe and is now the most severely affected one. The World Health Organization (WHO) reported 74,346 laboratory-confirmed cases in Europe on March 18 — 35,713 of them in Italy.
Figure 1 .

Our own hospital is highly contaminated, and we are far beyond the tipping point: 300 beds out of 900 are occupied by Covid-19 patients. Fully 70% of ICU beds in our hospital are reserved for critically ill Covid-19 patients with a reasonable chance to survive. The situation here is dismal as we operate well below our normal standard of care. Wait times for an intensive care bed are hours long. Older patients are not being resuscitated and die alone without appropriate palliative care, while the family is notified over the phone, often by a well-intentioned, exhausted, and emotionally depleted physician with no prior contact.
But the situation in the surrounding area is even worse. Most hospitals are overcrowded, nearing collapse while medications, mechanical ventilators, oxygen, and personal protective equipment are not available. Patients lay on floor mattresses. The health care system struggles to deliver regular services — even pregnancy care and child delivery — while cemeteries are overwhelmed, which will create another public health problem. In hospitals, health care workers and ancillary staff are alone, trying to keep the system operational. Outside the hospitals, communities are neglected, vaccination programs are on standby, and the situation in prisons is becoming explosive with no social distancing. We have been in quarantine since March 10. Unfortunately, the outside world seems unaware that in Bergamo, this outbreak is out of control.
Western health care systems have been built around the concept of patient-centered care, but an epidemic requires a change of perspective toward a concept of community-centered care. What we are painfully learning is that we need experts in public health and epidemics, yet this has not been the focus of decision makers at the national, regional, and hospital levels. We lack expertise on epidemic conditions, guiding us to adopt special measures to reduce epidemiologically negative behaviors.
For example, we are learning that hospitals might be the main Covid-19 carriers, as they are rapidly populated by infected patients, facilitating transmission to uninfected patients. Patients are transported by our regional system,1 which also contributes to spreading the disease as its ambulances and personnel rapidly become vectors. Health workers are asymptomatic carriers or sick without surveillance; some might die, including young people, which increases the stress of those on the front line.
This disaster could be averted only by massive deployment of outreach services. Pandemic solutionsare required for the entire population, not only for hospitals. Home care and mobile clinics avoid unnecessary movements and release pressure from hospitals.2 Early oxygen therapy, pulse oximeters, and nutrition can be delivered to the homes of mildly ill and convalescent patients, setting up a broad surveillance system with adequate isolation and leveraging innovative telemedicine instruments. This approach would limit hospitalization to a focused target of disease severity, thereby decreasing contagion, protecting patients and health care workers, and minimizing consumption of protective equipment. In hospitals, protection of medical personnel should be prioritized. No compromise should be made on protocols; equipment must be available. Measures to prevent infection must be implemented massively, in all locations and including vehicles. We need dedicated Covid-19 hospital pavilions and operators, separated from virus-free areas.
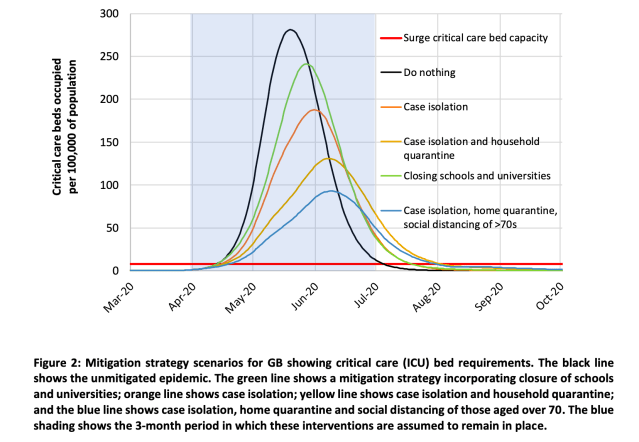
This outbreak is more than an intensive care phenomenon, rather it is a public health and humanitarian crisis.3 It requires social scientists, epidemiologists, experts in logistics, psychologists, and social workers. We urgently need humanitarian agencies who recognize the importance of local engagement. WHO has declared deep concern about the spread and severity of the pandemic and about the alarming levels of inaction. However, bold measures are needed to slow down the infection. Lockdown is paramount: social distancing reduced transmission by about 60% in China. But a further peak will likely occur when restrictive measures are relaxed to avoid major economic impact.4 We strongly need a shared point of reference to understand and fight this outbreak. We need a long-term plan for the next pandemic.
Coronavirus is the Ebola of the rich and requires a coordinated transnational effort. It is not particularly lethal, but it is very contagious. The more medicalized and centralized the society, the more widespread the virus. This catastrophe unfolding in wealthy Lombardy could happen anywhere.